CDC Webinar: Medetomidine
August 7, 2025
Dr. Jeanmarie Perrone and Dr. Samantha Huo speak on the clinical implications of medetomidine mixed with opioids seen in Philadelphia and nearby region of Southeast Pennsylvania.
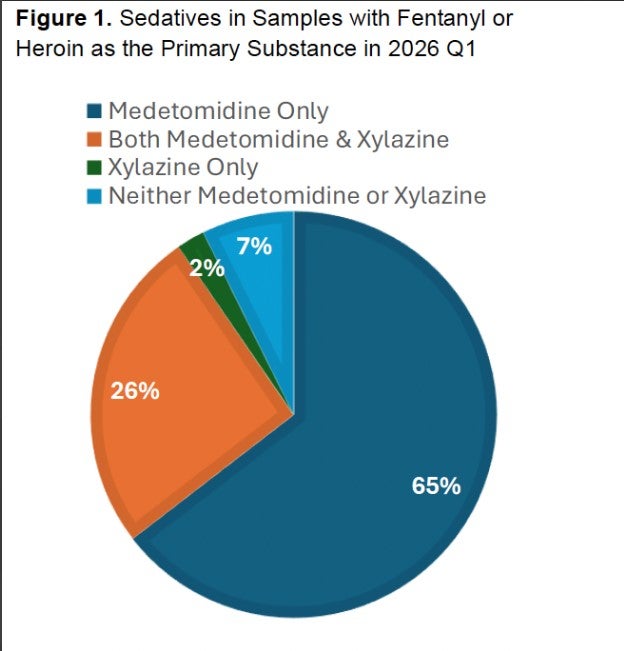
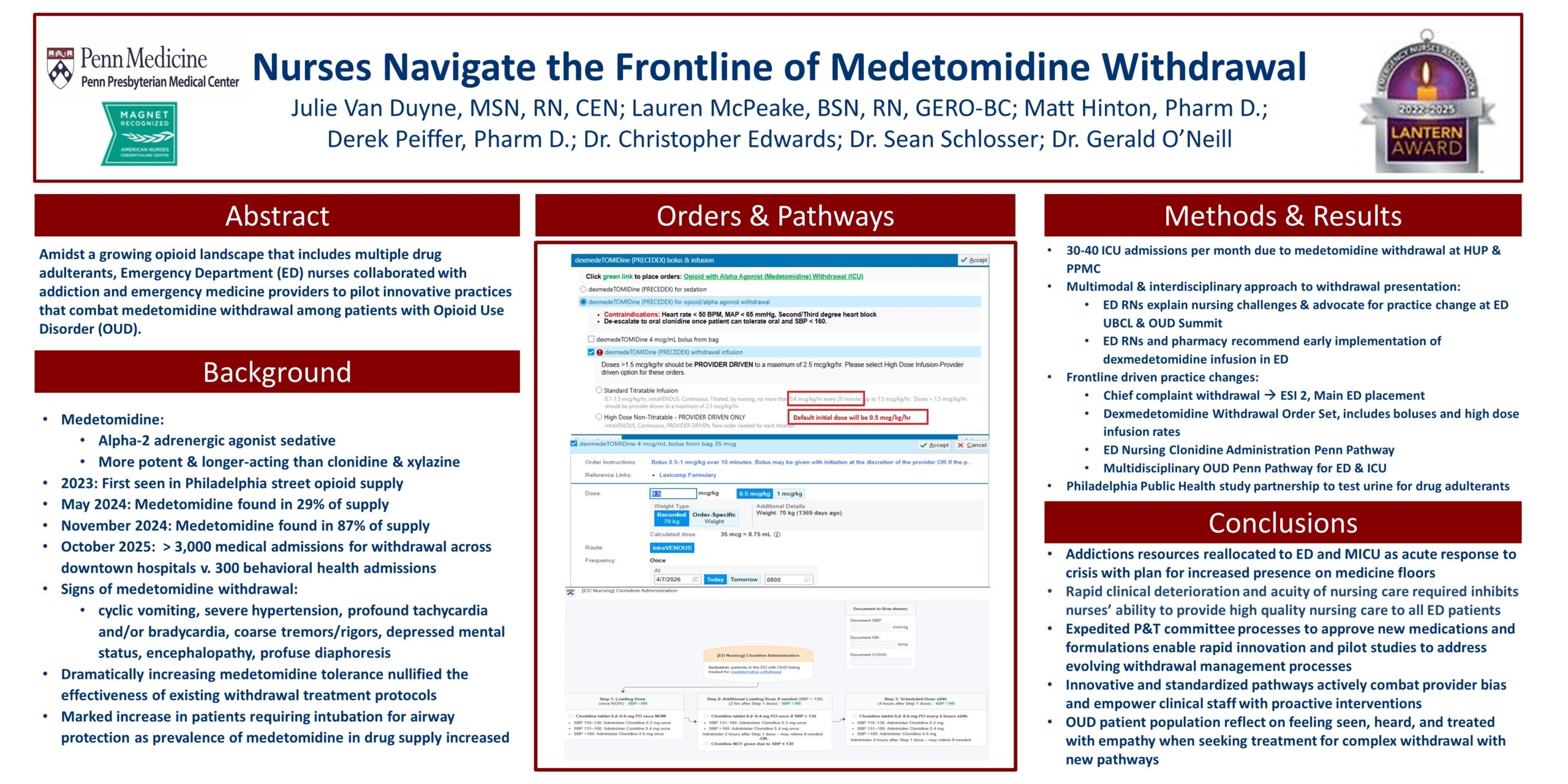
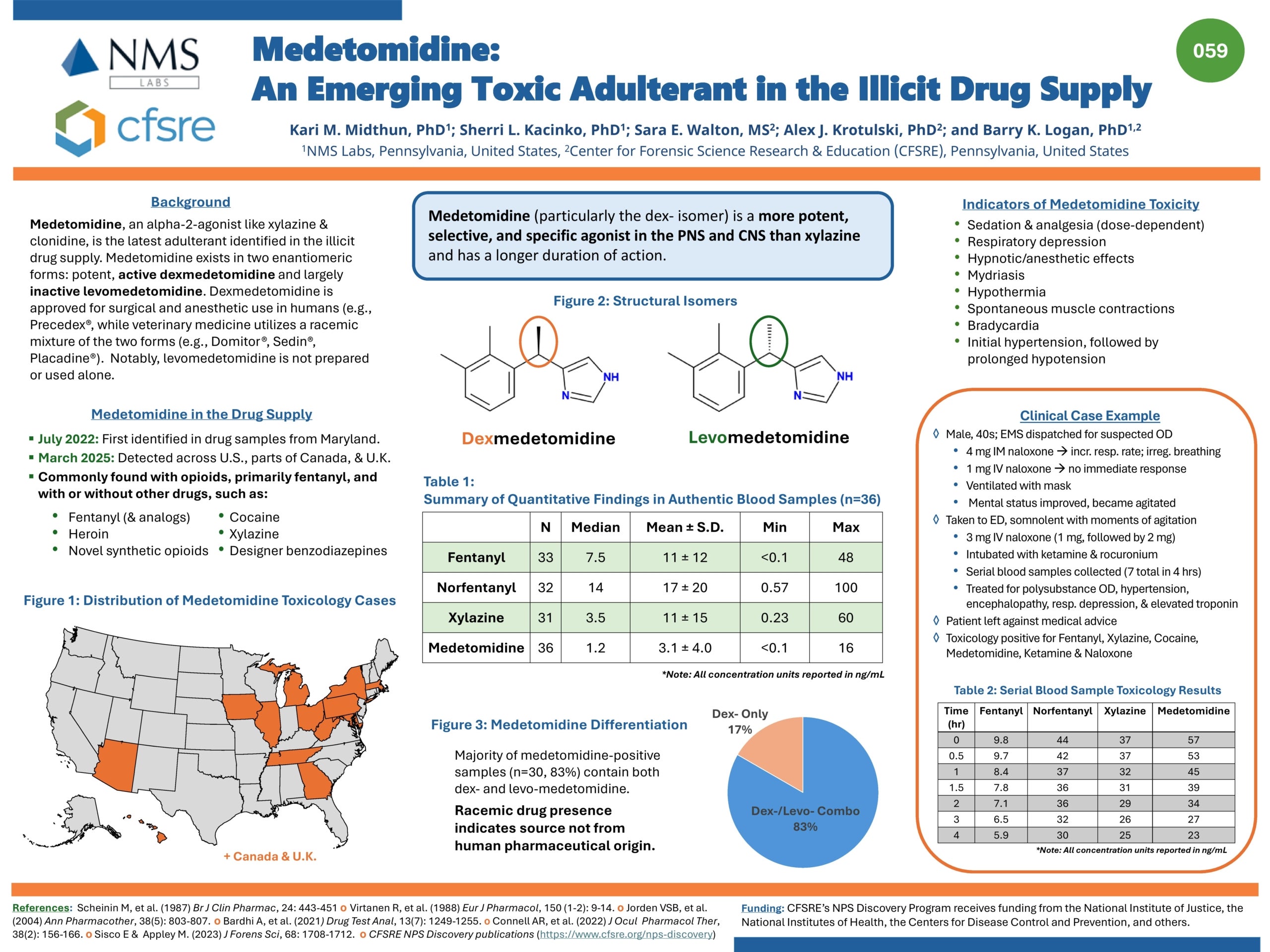
Medetomidine, an alpha-2 agonist not approved for human use, is an emerging drug adulterant that was found in 72% of illicit opioid samples by Philadelphia street drug checking programs in Q4 2024. During the same time frame, detection of xylazine (previously the most common adulterant), decreased from 98% to just 31% of samples. This represents a large shift in the regional opioid supply, one which has caused significant changes in the presentation of patients experiencing opioid overdose and withdrawal. It is important to note that fentanyl remained present in 100% of tested samples during this time period.
You can download our ICU medetomidine-fentanyl withdrawal management strategy here.
Recommended Medication Regimen (updated 9/11/25)
Note: Degree of alertness will influence regimen. Opioid administration should be prioritized.
(1) Long and short-acting opioid
Rationale: High quantities of fentanyl remain prevalent in the illicit opioid supply
(2) Dexmedetomidine (in lieu of clonidine)
Rationale: Drug checking reports a high prevalence of medetomidine in the illicit opioid supply
(3) Ketamine
Rationale: Regionally supported (addiction medicine) adjunctive in patients using fentanyl and/or xylazine
(4) Olanzapine
Rationale: Antiemetic and agitation treatment, may be particularly helpful in patients using xylazine and/or medetomidine
(5) Antihypertensive agents
Rationale: Severe hypertension may persist despite aggressive treatment with the above therapies. Earlier initiation is warranted if the patient has end organ dysfunction (hypertensive emergency).
(6) Additional adjunctive medications
Primary Care Physicians: Certificate for this course is hosted by the Health Federation of Philadelphia’s SURGE program with Dr. Judy Chertok and Dr. Rachael Truchil.

An Episode from the ASAM Podcast Series called Practice Pearls
February 9, 2026
Drs. Stephen Taylor and Jeanmarie Perrone follow up on Season 1’s episode, “Emerging Illicit Substances: What Clinicians Need to Know.” Together, they discuss how medetomidine has continued to spread to different regions and what has changed over the past year. They explore strategies for managing medetomidine withdrawal, keeping patients safe, and preparing for this growing public health threat.
Listen to the full episode here.
Dr. Jeanmarie Perrone and Dr. Samantha Huo speak on the clinical implications of medetomidine mixed with opioids seen in Philadelphia and nearby region of Southeast Pennsylvania.
May 1, 2025
Our providers at Penn Medicine collaborated with partners at Temple Health and Jefferson University Hospital to illuminate the need for testing medetomidine in other regional drug supplies.
![]()
The Center for Addiction Medicine and Policy joins the conversation with the City's Department of Public Health and colleagues from Thomas Jefferson Hospital and Temple University to discuss the latest findings on medetomidine, an adulterant that has been prominent in the drug supply.
![]()
Penn primary care provider discusses the rapid changes in the illicit drug supply, including additives and contaminants along with the profound clinical impacts in the American Family Journal editorial.
Read full article here.
![]()
June 22, 2026
View the entire PDF here.